When the constraint is people
The policy is real, the targets are real, and none of them touch a patient until the workforce is in place. Our reading of the neighbourhood health shift, and why it is a workforce question before anything else.

The NHS has spent two decades talking about shifting care closer to home. The 10 Year Health Plan, the Neighbourhood Health Framework, and the March 2026 contracting guidance now turn that talk into structure, targets and money. The policy architecture is, for the first time, real.
But policy architecture does not see patients. People do. And the question that runs underneath every neighbourhood ambition, the one that determines whether any of it actually happens, is a workforce question. Who staffs the neighbourhood teams? Who holds the relationships the model depends on? Who builds the capability when it does not yet exist?
This is our reading of where the workforce challenge actually sits, and what it takes to meet it.
The shift in one sentence
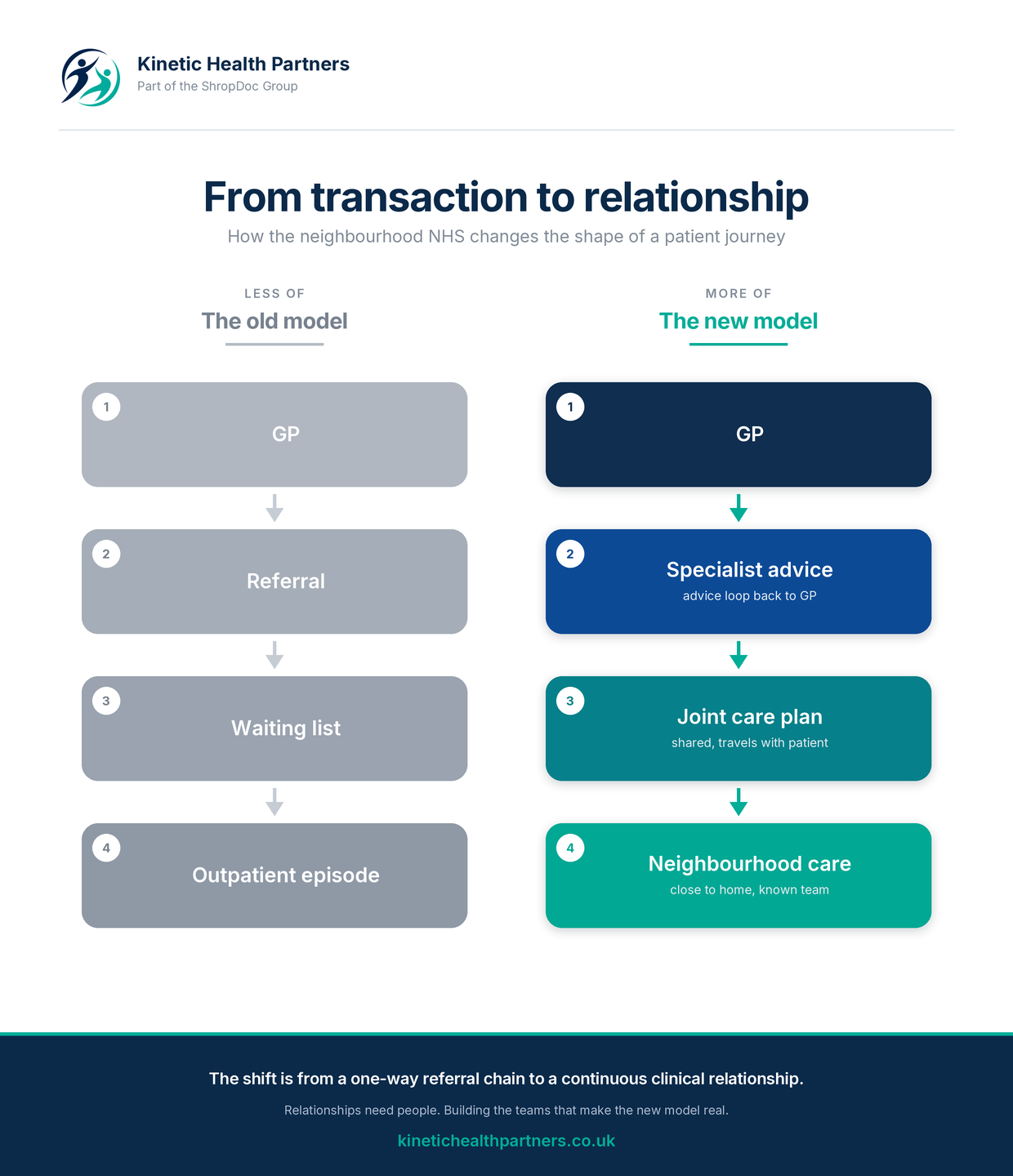
The neighbourhood model replaces a one-way referral chain with a continuous clinical relationship.
In the old model, a patient moves through a sequence of handoffs. GP to referral, referral to waiting list, waiting list to outpatient episode. Each step passes the patient to a new clinician who does not know them. The relationship resets at every door. Success is measured at the point of discharge, then the patient is handed back.
In the new model, the relationship holds. A GP and a specialist work together before a referral is even made. Advice flows first. A joint care plan travels with the patient. Care is delivered in the neighbourhood, by a team that knows the person, not just the presentation.
The clinical logic is not subtle. The populations who use the NHS most, frail older people, those with several long-term conditions, care home residents, people approaching the end of life, are exactly the populations who suffer most when care fragments. For them, continuity is not a comfort. It is the intervention. Every handoff is a risk. Every reset loses information. Every new face rebuilds trust from nothing.
The policy is now real, and it has teeth
It is worth being precise about how much has changed, because the workforce implications follow directly from it.
The March 2026 guidance introduces three nested population-based contract models. Single Neighbourhood Providers deliver integrated team services within one neighbourhood. Multi-Neighbourhood Providers coordinate across several, hold risk and gain sharing arrangements, and fill the gaps single providers cannot. Integrated Health Organisations hold a whole-population health budget for a defined geography and carry responsibility for the entire care pathway. The first wave of eligible providers is being designated now.
Alongside the contracts come hard national targets. A twenty-five per cent outpatient diversion rate for at least ten high-volume specialties by March 2027. A ten per cent reduction in follow-up appointments over the same period. A ten per cent reduction in non-elective admissions and bed days for frailty, care home, housebound and end-of-life cohorts by March 2029. These are not aspirations. They are measured commitments with money attached.
The evidence that the targets are achievable is genuinely strong. Analysis in Coventry and Warwickshire found that thirty-seven per cent of older people could avoid a hospital attendance, thirty-eight per cent could avoid admission, and forty-three per cent could be discharged earlier, all through better community access and coordination. The Strategy Unit found that up to a third of emergency admissions are potentially mitigatable. A neighbourhood of fifty thousand people generates over twenty-seven thousand first outpatient appointments and more than fifty thousand follow-ups a year, much of which advice-first models can reduce or remove.
The opportunity is real. The targets are real. What stands between them is the workforce.
Why workforce is the binding constraint
Every serious analysis of neighbourhood health arrives at the same bottleneck and then tends to move past it quickly, because it is the hardest part. We want to stay on it, because it is the part we exist to solve.
Three things make the workforce the constraint.
First, the model needs a different shape of clinician, not just more of the same. The balance between generalist and specialist has to shift. Deep specialist knowledge remains vital, but the ability to manage complexity and multimorbidity, to treat the whole patient rather than one organ system, becomes the scarce skill. Community nursing in many places has splintered into narrow specialist teams, frailty, end of life, chronic disease, wound care, catheters, each making separate visits with separate handoffs. The model calls for more holistic roles, held together by a smaller specialist core. That is a workforce design problem before it is a recruitment problem.
Second, the relationships the model depends on take time to build and are easily lost. The single most effective version of advice-first working is not an anonymous online consultant answering a query. It is a named specialist in continuing dialogue with a GP who knows them. That kind of relationship cannot be procured in a fortnight or stood up with locum cover. It is built by people who stay. Which means retention is not a workforce nicety. It is the precondition for the entire model.
Third, the financial and contractual mechanisms actively work against substantive staffing unless someone designs around them. The honest barrier, well understood and rarely solved, is that preventing an admission does not remove the ward or the staff who run it. The fixed cost is stranded. And at the front door, a hard-pressed admitting clinician choosing between admitting a patient and arranging to send them home safely will, rationally, often admit. It is less work and less risk. Bending that behaviour requires senior decision-making, alternatives to admission that genuinely exist, and teams positioned to catch the patient on the other side. All of which is, again, a workforce question.
The clinician's job itself is changing
This is the part that matters most, and it is the part most workforce planning has not caught up with.
Specialists working with neighbourhoods requires a major recasting of consultant job plans. The time-based job planning model the NHS has used for twenty years may need to give way to outcomes-based and population-health-based models. A diabetes consultant may come to hold accountability for glycaemic control and admissions across the population the hospital serves, not just for the patients who happen to reach their clinic.
As one analysis of the shift put it, just seeing more patients is not what is required. Seeing fewer for longer, to sort out the difficult problems properly, will generally add more value. That single sentence overturns the productivity logic the acute system has run on for a generation. It means the measure of a good clinical job stops being throughput and starts being contribution to a population's health.
This is a workforce shift before it is anything else. New job plans, a rebalancing of generalist and specialist skills, supervision structures that span organisational boundaries, and a definition of clinical value that the current contracts and performance regime were not built to reward. None of it happens without people who are recruited, deployed and retained against this new model rather than the old one.
Substantive over locum, every time
The workforce that makes neighbourhood health work is a substantive workforce. This is not an ideological preference. It is what the clinical model requires.
Locum cover has a place. It flexes capacity at the margin. But it cannot hold a relationship, cannot carry context across a fortnight, and cannot be the foundation of a continuity-first service for the populations that need continuity most. A locum-staffed neighbourhood service is a contradiction in terms. It churns the very relationships the model exists to protect.
Substantive recruitment, properly supported, also costs less over the life of a role than rolling locum cover, retains better, and delivers measurably better continuity. The financial case is straightforward once it is looked at over the right time horizon. The operational case is stronger still. The barrier is not whether substantive is better. It is that building a substantive workforce at pace, with the right governance, the right skill mix and the right supervisory structures, is genuinely hard, and most systems do not have the capability sitting idle to do it.
> Kinetic Resource builds substantive clinical teams for the neighbourhood NHS. [Find out more](/resource).
Where the workforce actually comes from
There are three sources, and a serious workforce strategy uses all of them rather than reaching only for the most visible one.
The first is redeployment. A significant part of the workforce already exists inside the system, working in configurations that pre-date the neighbourhood model. Community nurses, allied health professionals, pharmacists, paramedics, social care staff. Redeployment is faster than recruitment, but it carries governance, contractual and supervisory work that systems routinely underestimate, and it requires the simplification of overlapping community teams before it can be done well.
The second is recruitment. Real substantive recruitment into neighbourhood-shaped roles, not framework agency churn. The market for clinicians who want to work in community settings, with continuity, in genuine multidisciplinary teams, is tight but it is not empty. These clinicians exist and they are findable. What they will not respond to is a proposition that competes only on locum day rates. They are choosing a way of working, and the recruitment has to speak to that.
The third, and the most overlooked, is retention. Every clinician kept in post for another year is a clinician who does not need to be recruited. Most neighbourhood failure modes begin with workforce churn in the first six months after a service goes live. Investment in supervision, professional development, peer support and manageable caseloads is the single highest-leverage workforce intervention available to most systems, and it is consistently the one that gets cut first.
What good looks like
The workforce model that makes neighbourhood health real has three properties, and they hold together or they fail together.
It is clinically led. The decisions about team composition, supervision and cohort allocation sit with clinicians, not with procurement acting on their behalf. The neighbourhood lead clinician has genuine decision rights, because the people closest to the population are the people who understand what it needs.
It is jointly accountable. Workforce outcomes are shared between the system, the provider and the workforce partner. Continuity is measured. Retention is measured. The partner is accountable for whether the team holds and the population is served, not merely for the number of placements made.
It is neighbourhood-shaped. Roles are designed around the cohort, not the institution. Job descriptions reflect the population they serve, supervision reflects the team the clinician sits in, and career paths reflect the neighbourhood rather than the parent organisation. When these three properties are present, teams build and endure. When any one of them fails, the team comes apart inside eighteen months, regardless of how well it was recruited.
The role of a workforce and delivery partner
This is the work we do, and it is worth being clear about how a partner adds value, because the answer is not supplying people.
A workforce and delivery partner of the kind neighbourhood health needs does four things at once. It builds substantive teams against a defined population need, using recruitment, redeployment and retention together rather than reaching only for agency supply. It carries the operational and clinical governance from the first day, so that compliance is infrastructure rather than paperwork assembled in the final fortnight before a service goes live. It can operate a service directly where a system wants delivery rather than just staffing, holding the contract and the accountability for outcomes. And it brings the operating discipline, the mobilisation runbook, the supervisory structures, the iteration cadence, that turns a launched service into a sustainable one.
Kinetic Health Partners exists to do exactly this. We are a joint venture with ShropDoc, an organisation with thirty years of frontline community NHS delivery behind it. That heritage matters, because the operating model neighbourhood health describes is not theoretical to ShropDoc. Out-of-hours, urgent community response, care home support, vaccination at scale, these are services it has run for three decades across Shropshire, the West Midlands border and Mid Wales. What we add is the commercial platform, the national workforce capability and the operating discipline to extend that model into systems that need to mobilise it at pace.
We recruit substantively into neighbourhood teams. We operate neighbourhood services in our own right through the joint venture. Same operating model, different sides of the table. Because the systems that make neighbourhood health work will not be the ones with the most resources. They will be the ones that treat workforce as the architecture, not the afterthought.
The decade ahead
There is a warning underneath the whole neighbourhood agenda, and it is worth stating plainly. After years of undelivered rhetoric about shifting the balance of care, the people leading this round of reform understand that if it fails this time, hospitals will face demand they cannot accommodate or staff. The model is not optional. The arithmetic of an ageing population with rising multimorbidity does not leave a version of the future where the current hospital-centric model simply expands to cope.
So the workforce question is not a detail of implementation. It is the question. The policy is real, the contracts are real, the targets are real, and none of them touch a patient until the people are in place to deliver them. Building those teams, substantively, with continuity, shaped around the neighbourhoods they serve, is the work of the decade.
That is the work we are here to do.
*Kinetic Health Partners is part of the ShropDoc Group. We recruit and operate clinical teams for the neighbourhood NHS. This article was prompted by the National Association of Primary Care publication Providers and Neighbourhood Health by Nigel Edwards (May 2026), which examines the same shift from the perspective of acute providers.* [*Talk to us about your workforce.*](/contact)


